Aetiology
Trauma
A. Ankle Fracture
Types
- Weber A 4%
- Weber C 33%
- Displaced large posterior malleolar
Any OA develops in first 2 years
Causes
- articular damage at time of injury
- non anatomical reconstruction
- complications i.e. infection
B. Plafond Fracture
C. Talus Injury
Talar Dome OCD
Talus AVN
Talar neck malunion
Other
Inflammatory OA
Infection
Hemochromatosis
Hemophilia
Charcot
Incidence
Ankle OA much lower than hip or knee
Anatomy
Thin cartilage 1 mm
Joint highly congruent
Tibio-talar contact stresses
- 1mm shift causes 40% decrease in contact area
- medial instability more important than lateral instability
Clinically
Pain
- with weight bearing
- nightime
Stiff Ankle Joint
Xray
Ranges from
- anterior spurring
- severe OA




CT
Useful to define small anterior osteophytes
- may be causing pain with excessive dorsiflexion

MRI



Management
Non Operative
Solid Ankle Foot Cushion (SACH) + rocker bottom sole
Analgesia
HCLA / Hyaluronic acid Injections
Operative Options
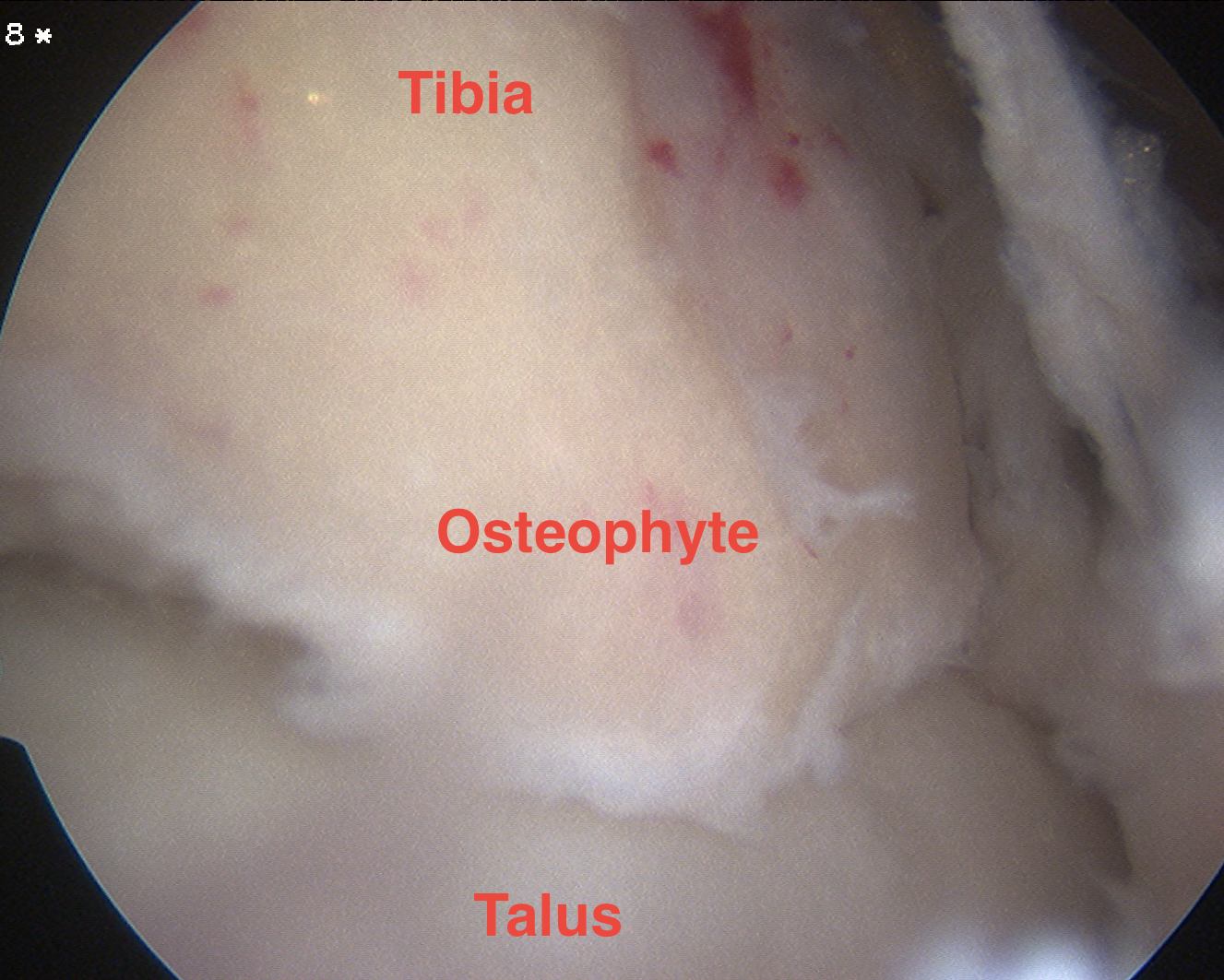
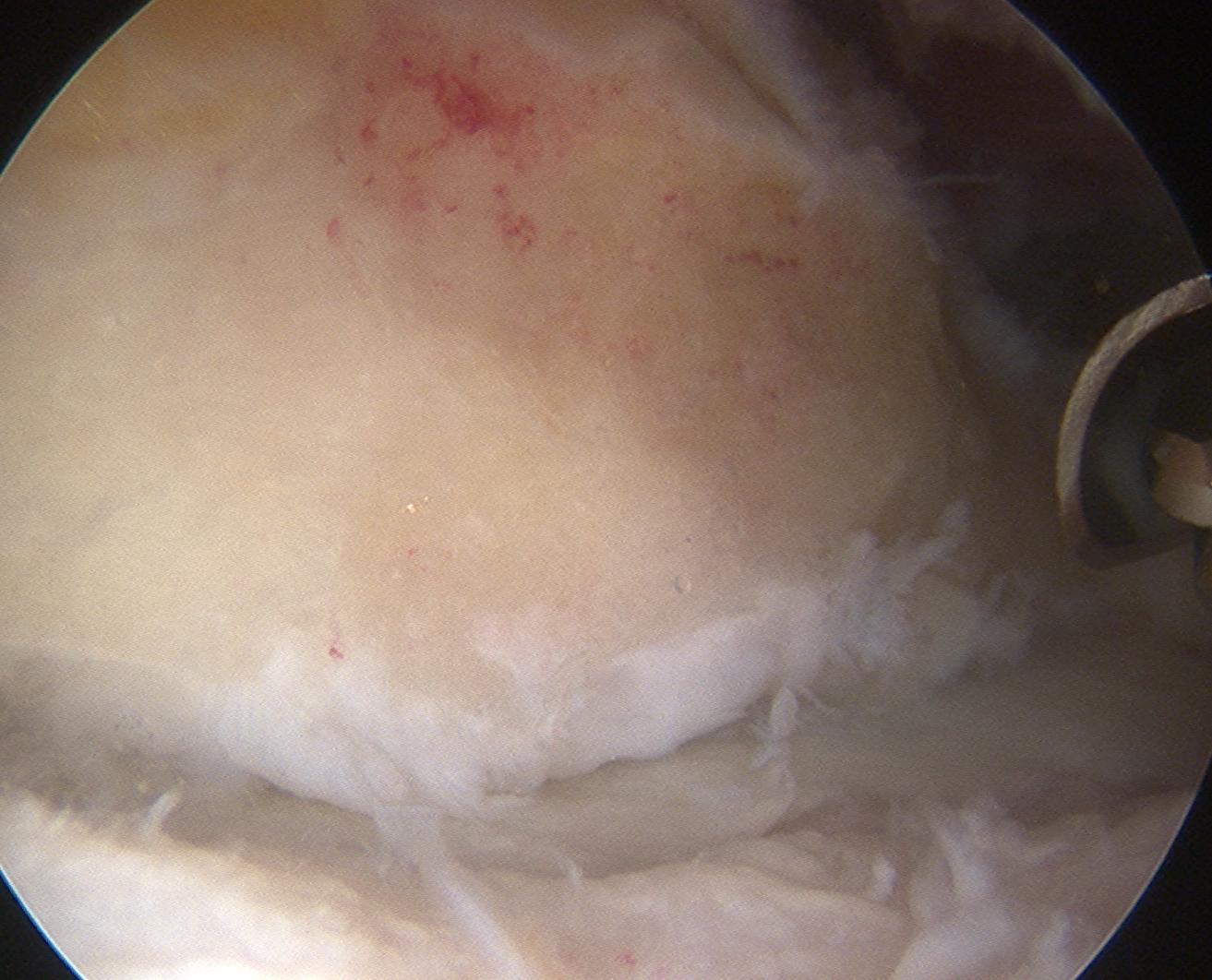
1. Arthroscopic debridement
Technique 1
- debride chondral lesions
- microfracture / abrasion
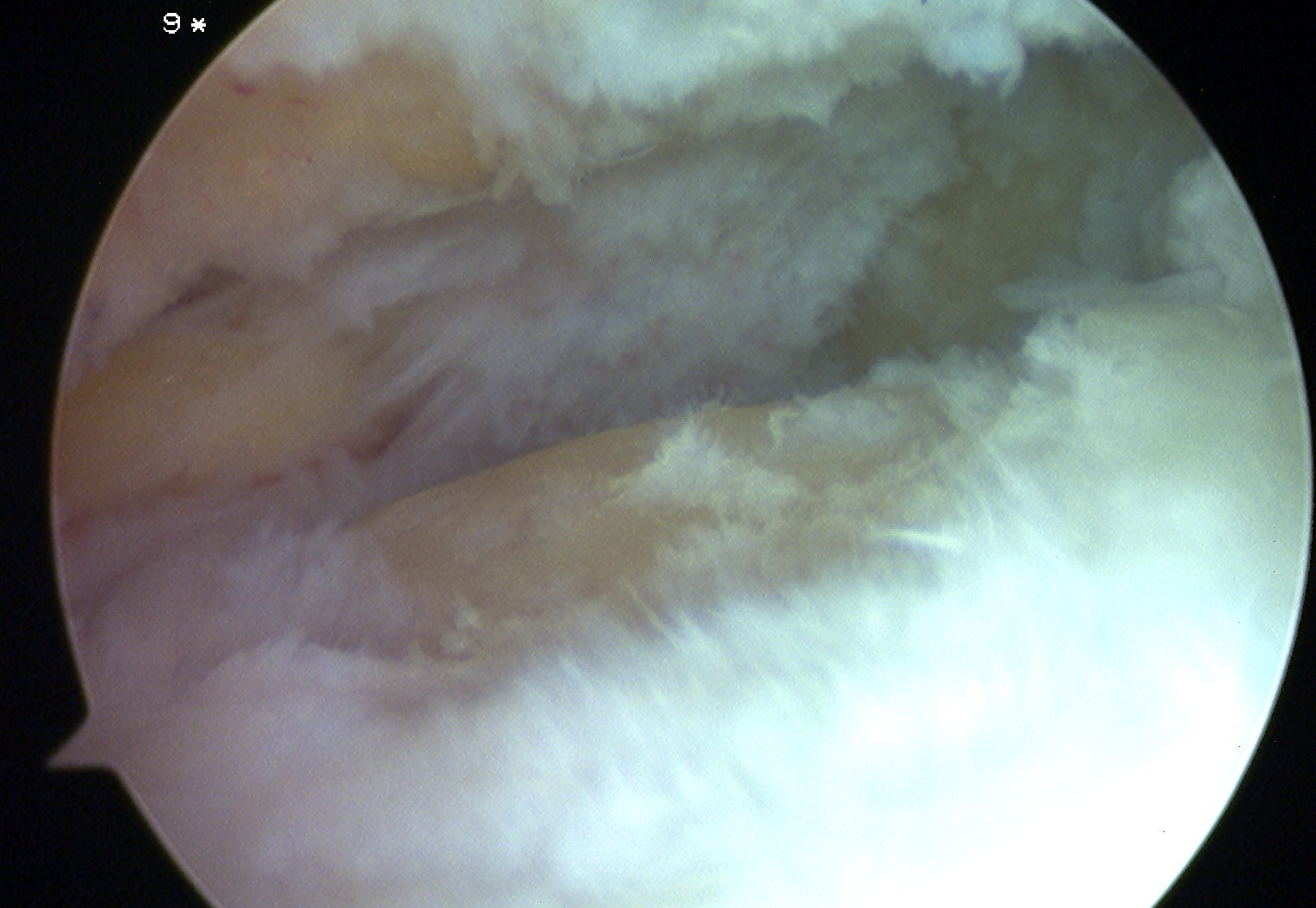
Technique 2
- removing kissing osteophytes
- anterior tibial and talar neck osteophytes

2. Articular distraction with external fixator
Technique
- apply for 4/12
- distracted 5 mm
- reasonable results reported
- up to 3 years improvement
- delays arthrodesis
3. Ankle Arthrodesis
4. Ankle Replacement